[www.medicalnewstoday.com]
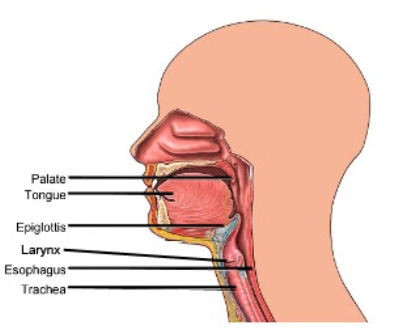
Epiglottitis is inflammation (swelling) of the epiglottis - a flap located at the base of the tongue which stops food from going down the wrong way into the windpipe (trachea), when we are eating. As the epiglottis sits in a crucial place for proper breathing, if it becomes swollen it can cause serious breathing difficulties and is treated as a medical emergency. In some cases, epiglottitis can completely close off the windpipe and the patient cannot breathe, known as respiratory failure.
If left untreated, epiglottitis symptoms can worsen quickly and the patient can die within a matter of hours.
If left untreated, epiglottitis symptoms can worsen quickly and the patient can die within a matter of hours.
Since the introduction of the Hib vaccine (Haemophilus influenzae type B vaccine), the number of epiglottitis cases has dropped dramatically. Epiglottitis used to be a widespread infection among young children before the Hib vaccine. As bacteria other than type b Hib can cause a similar inflammation, cases of epiglottitis still exist. In the UK there is 1 case in every 200,000 children and 1 in every 100,000 adults each year now.
What are the signs and symptoms of epiglottitis ?
A symptom is something the patient reports and feels, while a sign is something other people, including a doctor may detect. For example, a headache may be a symptom, while a rash may be a sign.An affected patient, often a child in some developing nations that don't have widespread Hib vaccinations, may experience :
- Fever
- Swallowing difficulties, often painful
- Drooling
- A hoarse or muffled voice
- Stridor - a high pitched sound that accompanies respiration, especially when breathing in
- Severe sore throat
- Cyanosis - skin may take on a blue tinge if the patient is not getting enough oxygen
What causes epiglottitis ?
- Hib bacteria (Haemophilus influenzae type b) - infection can cause epiglottitis as well as meningitis and pneumonia. Since widespread vaccinations, incidence of epiglottitis has dropped dramatically.
- Other bacteria - such as the one that commonly causes pneumonia - streptococcus pneumoniae.
- Fungi - especially individuals whose immune systems are weak.
- Chickenpox.
- An injury - if you swallow a very hot drink too quickly there is a risk that the epiglottis will swell. Other injuries, caused by a blow to the neck may also cause epiglottitis.
How is epiglottitis diagnosed ?
The medical team will focus on making sure the patient has an adequate supply of oxygen if epiglottitis is suspected, before any diagnostic tests are considered.Risk Factors
Epiglottitis is a contagious disease. It is passed much like the common cold , through droplets released when sneezing and coughing. Anyone can develop epiglottitis, however the following factors can increase a person’s risk :
- Age :
- Children, aged 3-7, living in countries that do not offer vaccines
- Infants too young to receive vaccination (younger than two months)
- Adults in their 40s (very rare)
- Sex : Males are more prone than females
- Living in close quarters
- Attending day care, being in school, or working in an office
- Weather : more common in winter
- Race : more common among African Americans and Hispanics
Treatment
The doctor will first stabilize your airway and then give proper medication depending on the cause. You may also have secondary illnesses that need to be treated depending on the cause of the epiglottitis (eg, blood infections due to Streptococcus ).
If you CAN breathe, you will be closely monitored in the intensive care unit.
If you CANNOT breathe, the options include :
- Endotracheal intubation—A breathing tube is inserted through the nose or mouth and fed into the airway. This can only be done if the airway is not swollen shut and should be done by an experienced physician.
- Tracheotomy —A breathing tube is inserted directly into the trachea (airway). This is done if the airway is swollen shut, or if the airway is too swollen to do an endotracheal intubation.
After the airway is stabilized, you will be monitored and started on medications, including :
- Antibiotics—Antibiotics given through the veins (IV) help kill the organism causing the infection and swelling. At first, a variety of antibiotics may be given if the identity of the germ is not yet known. Once the laboratory test results are known, a specific antibiotic can be given.
Once swelling decreases, the breathing tube can be removed. Usually, there are not any lasting side effects of epiglottitis, and the outlook is good.
What are the complications of epigliottitis ?
The most dangerous complication is respiratory failure (the patient cannot breathe properly, and sometimes not at all) - this is a life-threatening condition.An infection can spread and otitis media (inner ear infection), meningitis, pericarditis (heart lining infection) and pneumonia can develop.
Diagnosis
When you arrive at the hospital, the doctor will first make sure you are able to breathe. Once this is affirmed, the doctor will ask about your symptoms and medical history. If you are not having trouble breathing, the doctor may use a mirror to look down your throat. Usually, initial diagnosis and testing are based on the reported symptoms.
Tests that may be run include :
- Neck x-ray —a test that uses radiation to take a picture of the neck, so the doctor can check for a swollen epiglottis
- Blood culture—to screen for bacteria
- Blood count—to document presence of bacterial infection
- Nasolaryngoscopy—a tiny, lighted tube inserted through the nose to look at structures like the epiglottitis
- Throat culture—A cotton swab is used to collect cells from the infected tissue; the cells are plated on a nutrient-rich medium and allowed to grow. The cells are then identified, and the results are given to the doctor.
Prevention
Vaccination is the only way to prevent epiglottitis. There are three different vaccines that can be given (HbOC, PRP-OMP, and PRP-T). Currently, infants born in the US are given one of these vaccines at two months of age. Since vaccination began, adults have been at even lower risk of developing epiglottitis. However, if you are immune compromised or on medications that may make you more susceptible to illness, speak with your doctor about the possibility of getting vaccinated. An antibiotic (ie, rifampin) may be prescribed for post-exposure coverage for :
- Household members and others who have spent time in the previous 5 out of 7 days with an affected individual
- All day care staff
No comments:
Post a Comment